Glaucoma Treatments
Glaucoma Treatment in Shelton, CT

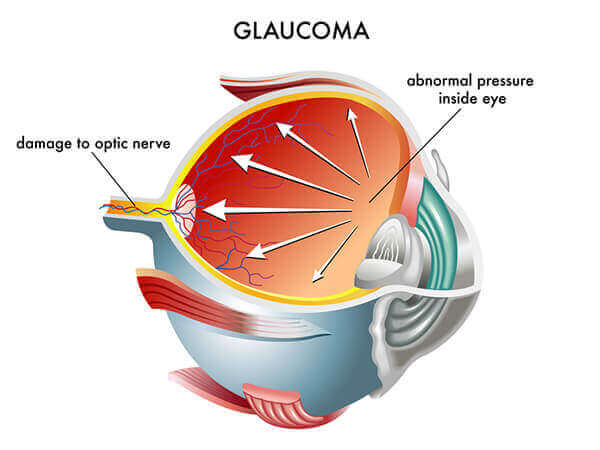
Glaucoma is a disease in which there is damage to the optic nerve, usually resulting from chronically high pressures inside the eye. The optic nerve receives the visual image from the retina and sends the image to the brain. The brain interprets this image as sight. Some patients have glaucoma, even though their pressure is “normal.” These patients have “low tension glaucoma.” Their optic nerves have an increased susceptibility to damage and need to have their eye pressure lower than normal to prevent progression of damage.
Who has glaucoma? Who is at risk?
Glaucoma is the second leading cause of blindness in the U.S., affecting over 3 million Americans. Anyone can develop this pervasive eye disease. Some groups are at higher risk than others, including: African Americans over age 40; everyone over age 60, especially Mexican Americans; and people with a family history of glaucoma.
What are some symptoms of glaucoma?
Glaucoma usually happens in both eyes, often affecting one eye more than the other. In the early stages, no vision loss is noted by the patient. Patients are totally unaware that they have the condition; hence the term, “Sneak thief of sight.” The other reason that people are often unaware that they are developing glaucoma damage is that, since the disease tends to worsen very slowly, patients tend to “adapt” to the changes and are not aware that their peripheral vision isn’t as bright as it was five years earlier.
In typical chronic open angle glaucoma, there is no pain, redness or other symptoms that might alert patients to their problem. Specialized testing at our office including OCT, pachymetry, disc photography and automated visual fields may detect early peripheral visual field loss, or subtle damage to the optic nerve. It is rare, however, for patients to notice these peripheral vision changes until the condition is quite advanced. Some patients may notice difficulty with dark adaptation and loss of contrast sensitivity. If your IOP (intraocular pressure) remains high, peripheral vision loss may eventually become noticeable, and in advanced disease, central vision will be lost. By the time central vision is lost, the disease is very advanced. Unfortunately, any damage that has already occurred cannot be restored. The goal of glaucoma care is to prevent patients from ever developing advanced damage and loss of sight. Glaucoma is a potentially serious disease. However, glaucoma seldom causes complete blindness when detected and treated early.
In contrast to painless, progressive chronic open angle glaucoma, five to ten per cent of people with glaucoma have a particular type of glaucoma known as angle closure glaucoma. People with this condition need to avoid taking certain medications such as antihistamines and anti-nausea medicines that can precipitate an “attack.” An angle closure attack can cause a patient to present with sudden pain, nausea, headache, halos around lights and visual loss. Eye pressure is typically very high, perhaps four or five times the normal eye pressure. Urgent treatment, usually a treatment called laser iridotomy is required to cure the attack.
How is glaucoma treated?
The best way to combat glaucoma is prevention, and that comes from early diagnosis and treatment. A thorough eye examination by an Ophthalmologist is the only way for you to know if you have this initially asymptomatic, yet progressive condition. The main initial treatment strategy is eye drop medication or laser. At The Pinke Eye Center in Shelton, CT , we individualize treatment for each patient and monitor the effectiveness of treatment on an ongoing basis. Some patients do better with initial laser treatment, some do better with eye drops, and some need a combination of treatments. Some patients have more advanced disease that requires outpatient operating room surgery. James R. Pinke, M.D. sees all of his patients at every visit and performs all treatments and surgical procedures himself. He believes that this continuity of care provides his patients with the highest quality treatment both short and long term. At the Pinke Center for Eye Heath, patients can be assured that they will not be directed to see an optometrist or other eye care professional that they didn’t expect to see that day.
What are the surgery options for glaucoma?
If you think of glaucoma as a problem in which the internal eye fluid cannot escape well causing the pressure to increase, then this will make it easy to understand the laser procedures. Think of a sink, which has a faucet and a drain. If the faucet is pouring too much water into the sink, it overwhelms the drain and the sink fills up, even if the drain is open. On the other hand, if the drain is clogged, then even a normal amount of water coming from the faucet fills the sink. In glaucoma, both problems can exist separately or simultaneously. Some of the treatments slow down the faucet, and some of the treatments help open the drain. In the eye, the faucet is a structure behind the iris (colored part of the eye) called the ciliary body. The drain is in the angle of the eye formed by the connection of the iris to the inner wall of the eye, the trabecular meshwork. Eye drops, laser surgery and glaucoma surgery all work on either the faucet or the drain, or both.
James R. Pinke, M.D. offers several laser surgical procedures for glaucoma as well as standard trabeculectomy surgery, express mini shunts and iStent for advanced glaucoma that cannot be controlled with medications or laser. Most of the laser surgery is performed at the Shelton office, while some laser procedures are conducted at the Connecticut Eye Surgery Center.
What is Selective Laser Trabeculoplasty (SLT)?

James R. Pinke, M.D. was one of the first ophthalmologists in Connecticut to offer Selective Laser Trabeculoplasty (SLT) for the treatment of Open Angle Glaucoma. To use the analogy in the prior paragraph, SLT helps to open the drainage channel of the eye known as the trabecular meshwork. This procedure has largely replaced Argon Laser Trabeculoplasty. The advantages of this newer laser include the fact that the procedure is painless and that it can be performed repeatedly. In fact, James R. Pinke, M.D. has had excellent success with this laser and now offers this as initial treatment for patients who would like to avoid drops. There are virtually no side effects, no recovery, no pain virtually no complications. There is no incision, and no post-operative restrictions, and it is performed right in his Shelton office. Unfortunately, like all glaucoma care, no treatment works for all patients. James R. Pinke, M.D. has performed well over one thousand SLT procedures over the past four years since 2002.
What is ECP (Endoscopic Cyclo-Photocoagulation)?
Another laser procedure, performed in the operating room is called ECP (Endoscopic Cyclo-Photocoagulation.) This procedure often lowers pressure quite effectively. ECP is a laser treatment to the ciliary body, which is located behind the iris. The laser reduces the amount of fluid that the eye is producing, thus lowering the pressure in the eye. ECP is performed at the Connecticut Eye Surgery Center, one of the only places in Connecticut to offer this advanced procedure. James R. Pinke, M.D. was one of first Ophthalmologists in Connecticut to offer this procedure. ECP requires a small incision into the eye. The laser probe is then passed under the iris, and the ciliary body is treated with the endoscopic laser. This procedure is usually performed in glaucoma patients in conjunction with cataract surgery, through the cataract incision, after the cataract operation is complete. It adds five or ten minutes to cataract surgery. ECP lowers intraocular pressure and often reduces or eliminates need for glaucoma drops. It can also be performed as a “stand alone” procedure in glaucoma patients who have had prior cataract surgery.
Many patients benefit from SLT and ECP. The two procedures work on different parts of the eye; SLT treats “the drain,” while ECP treats “the faucet.”
What is Laser Iridotomy?
Angle closure glaucoma and patients who are at risk for angle closure glaucoma are treated in the office or the surgery center with laser iridotomy. In angle closure glaucoma the space between the drainage portion of the eye (the trabecular meshwork), and the iris is very narrow. When this space suddenly closes off, there is a sudden, severe pressure rise, which can lead rapidly to blindness. In this case, the drain isn’t just partially clogged; it is suddenly, completely blocked. The internal eye fluid has nowhere to go. This causes a dangerous pressure build up. Laser Iridotomy is a technique in which a tiny hole is made in the iris, allowing fluid to escape to the front part of the eye, opening the drainage channels and instantly curing this type of glaucoma. This procedure has totally replaced prior emergency surgery, is painless, has no side effects, and is curative.
Sometimes, the angle remains narrow even with a Laser Iridotomy procedure. This is a specific syndrome called Plateau Iris. In this situation, the angle can be deepened further by performing a laser treatment known as Argon Laser Iridoplasty, to “shrink” the iris away from the drainage area. This is also done right in the office, takes a few minutes, has no side effects, requires no post operative care and has no recovery period.
What is Trabeculectomy?
Finally, patients with advanced glaucoma that cannot be controlled with drops or laser may need operating room surgery. In these situations, the primary operation is called Trabeculectomy, in which a “trap door” opening is made in the wall of the eye to allow fluid to drain directly, thus dramatically reducing the eye pressure. This procedure is successful more than eighty percent of the time. Usually, the pressure can be lowered enough so that eye drops are no longer necessary following the post-operative recovery period. This outpatient procedure takes about thirty minutes in most cases, is done with local anesthesia and is performed either at the Surgery Center or at Griffin Hospital.
Located in Shelton, Dr. James Pinke is your Connecticut Glaucoma Surgeon Of Choice.
For more information or to schedule a Comprehensive Eye Exam with Glaucoma screening, Request an Appointment.

